

Oral Minoxidil vs. Topical Minoxidil — How to Choose, Read Through Systemic Exposure, Delivery to the Follicle, and the Role of Stem Cell Conditioned Media2026.07.09
“Oral minoxidil or topical minoxidil — which one should I actually be on?” This is a question we hear in almost every AGA consultation. Even though they share the same active ingredient, oral minoxidil and topical minoxidil differ substantially in how the drug reaches the body, how it acts at the follicle, and what side-effect profile comes with them. In recent years in particular, oral minoxidil — which is not approved in Japan for AGA and is used off-label — has spread through personal import and self-pay clinics, and the understanding of its safety and efficacy has not always caught up. In this article, our supervising physician organizes the differences between oral minoxidil and topical minoxidil, through the lenses of pharmacology, systemic exposure, and how stem cell conditioned media sits on a separate axis of regenerative medicine.
Key Points of This Article
・Oral minoxidil is a “systemic drug” that rides the whole circulation, while topical is a “local drug” that stays on the scalp — the delivery is fundamentally different.
・Oral minoxidil tends to feel effective, but risks of systemic side effects like hypertrichosis, edema, and palpitations are more likely to rise.
・Topical minoxidil has a thick body of long-term evidence and a wide safety window, but percutaneous absorption is a wall — how much reaches the follicle varies between individuals.
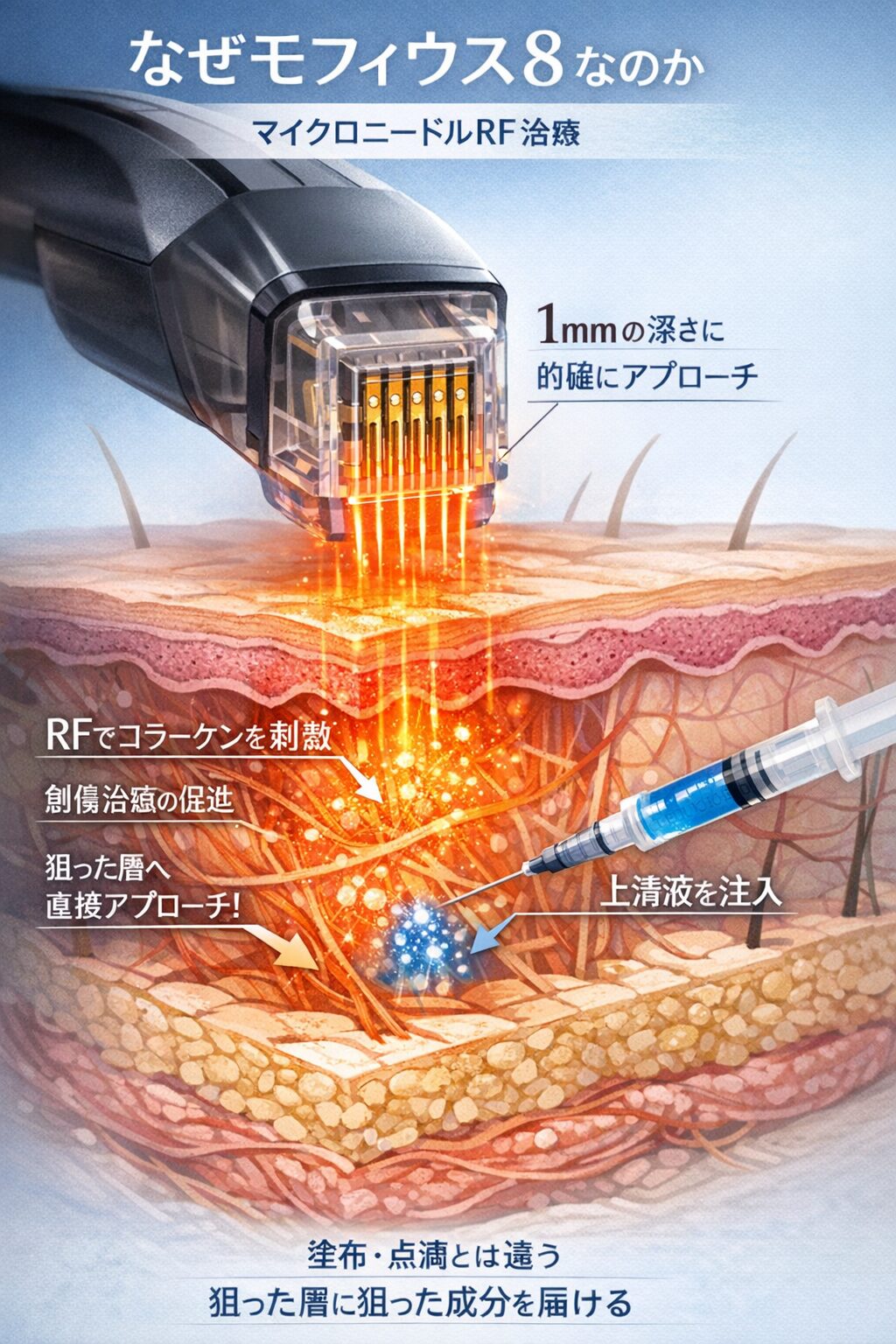
・Stem cell conditioned media is not a “replacement for minoxidil” but a different axis that tunes the follicular microenvironment, positioned for combination or as a bridge.
・Choice depends on progression, age, pregnancy planning, and systemic disease — the simple idea of “stronger drug is better” should be avoided.
What Is Minoxidil Actually Doing?
Minoxidil was originally developed as an oral vasodilator for severe hypertension. It opens ATP-sensitive potassium channels, relaxes smooth muscle, and widens peripheral blood vessels. During its development, hypertrichosis was observed as a side effect, and that observation led to its repositioning as a topical scalp drug.
Its mechanism in hair is still not fully understood. Proposed actions include improving blood flow around the follicle, driving VEGF production in dermal papilla cells, extending the anagen (growth) phase, and pushing hairs out of telogen — together nudging the follicle toward hair growth.
Oral Minoxidil vs. Topical Minoxidil: The Delivery Is Fundamentally Different
Oral Minoxidil Rides the Whole Circulation
Oral minoxidil is absorbed from the gut, metabolized in the liver, and carried by the bloodstream to follicles all over the body. It can reach the dermal papilla in the scalp at a high enough concentration and can act at deeper regions that topical struggles to reach — this is its biggest strength.
But it doesn’t only reach the scalp. Vellus hair on the face, trunk, and limbs receives the same signal, so facial hypertrichosis becomes a real problem in women, and men often notice thicker hair on the arms and back. The vasodilator effect itself is also systemic, so fluid retention, weight gain, elevated heart rate — and rarely pericardial effusion — are not zero.
Oral minoxidil is not approved for AGA in Japan. When it is used, it is off-label under self-pay care, and honest risk explanation, informed consent, and blood pressure / heart rate monitoring are non-negotiable responsibilities on the clinician’s side.
Topical Minoxidil Stays on the Scalp
Topical minoxidil is applied directly to the scalp and absorbed percutaneously into the follicle. Systemic exposure is orders of magnitude smaller than with the oral form, and the risk of systemic side effects like hypertrichosis, palpitations, and edema is relatively low. In Japan, 1%–5% preparations are approved as over-the-counter drugs, and long-term use evidence is well accumulated.
The weakness is the “percutaneous absorption wall.” How much crosses the stratum corneum and reaches deeper follicular layers varies between individuals, and the absorption rate shifts with scalp thickness, sebum level, stratum corneum condition, and vehicle (propylene glycol / alcohol / foam). Some of the “I’m applying it but nothing happens” cases can be explained by this delivery gap.
How to Think About the Trade-Off Between Effect and Side Effects
Oral can pull additional response out of cases that plateaued on topical. When AGA has progressed to Norwood IV–V and twelve months of topical use has not produced a clear change, adding or switching to oral becomes worth considering.
But its “punch” comes at the price of riding the systemic circulation. Hypertrichosis is not easy to walk back, and fluid retention becomes a latent aggravator of heart failure and renal decline. Women who are planning pregnancy, currently pregnant, or breastfeeding do not use it as a rule. Anyone with cardiac or renal disease, or on antihypertensives, must share the hemodynamic implications with their primary physician.
Topical, by contrast, has a rich long-term safety dataset and over two decades of use. Most side effects stay local — itching, contact dermatitis, initial shedding — and are largely reversible on discontinuation. Starting with topical, watching the response for six to twelve months, and then designing the next step is currently the lowest-risk plan.
Stem Cell Conditioned Media as “A Separate Axis”
The clarifying point here is that stem cell conditioned media is not a “replacement” for minoxidil, but a separate axis. Minoxidil approaches through vasodilation and direct action on dermal papilla cells; stem cell conditioned media carries multiple growth factors (VEGF, IGF-1, HGF, KGF) and exosomes, and works on the inflammatory environment around the follicle, on angiogenesis, and on the follicular stem-cell niche.
For people who develop systemic side effects on oral minoxidil, for women who cannot use either oral or topical during pregnancy or breastfeeding, and for those who respond poorly to topical, scalp delivery of stem cell conditioned media through injection or drug delivery adds a new drawer to the toolbox. Combined with minoxidil, additive effects can be expected because the mechanisms differ, and conditioned media is also considered as a maintenance-phase option after minoxidil is tapered off.
Of course, stem cell conditioned media is not a cure-all. In advanced AGA where the follicles themselves are miniaturized or lost, restoring density with conditioned media alone is difficult. Within the whole architecture of AGA treatment, oral, topical, and regenerative therapies need to be arranged individually by “which order and which intensity.” See our column list on hair regenerative medicine for related articles from other angles.
The Choice Is Made by “Total Safety Design,” Not by “Which Punches Harder”
The question is not “which one works” but “how do risk and benefit balance out given this person’s life, systemic status, pregnancy plans, and progression.” Young man with mild AGA — start topical. Woman planning a pregnancy — oral is generally not used. Cardiac history — cardiovascular assessment must precede oral. Someone who wants to minimize systemic drug burden — the scalp-directed approach with stem cell conditioned media is one option.
For AGA treatment guidance and topical indications, the male- and female-pattern hair loss clinical practice guidelines published by the Japanese Dermatological Association are worth referring to. Because the balance between effect and safety is individual, we strongly recommend seeing a physician before deciding on personal import of oral minoxidil on your own.
Frequently Asked Questions
Q. Does oral minoxidil definitely work better?
Delivery to the follicle is better with the oral form, and even people who responded poorly to topical can improve. But because it rides the systemic circulation, the risks of hypertrichosis, edema, and cardiovascular effects go up, there is no “guaranteed to work,” and the side-effect profile is fundamentally different. Individual variability and careful indication remain the prerequisites.
Q. Does combining oral and topical give more effect?
Additive effects are theoretically possible, but side-effect risks also add up. Systemic fluid retention and hypertrichosis in particular tend to intensify, so combination should be judged under a physician’s management, weighing necessity against safety.
Q. Can women take oral minoxidil?
Low-dose regimens are used overseas, but it is generally contraindicated during pregnancy, breastfeeding, and pregnancy planning. Facial and body hypertrichosis is easier to develop, and the daily-life burden tends to be greater than in men, so cautious indication is required.
Q. Can I stop minoxidil if I use stem cell conditioned media?
Not necessarily. Because the mechanisms differ, realistic designs include using them together for additive effect, or using conditioned media as a bridge while aiming to reduce or discontinue minoxidil. The decision to stop is made individually while watching the course.
Q. Are there people for whom topical simply does not work?
Yes — response can be poor due to individual differences in percutaneous absorption, the stratum corneum barrier of the scalp, and the degree of follicular miniaturization. If three to six months of use shows no clear change, we reconsider the diagnosis and revise the treatment strategy.
──────────────
Supervising Physician: Shin Moriwaki, MD
Japan Society of Aesthetic Surgery (JSAS) Member / American Academy of Aesthetic Medicine Member
ECFMG Certificate (US Medical License Qualification)
──────────────
📍AVAN TOKYO Ginza Hair Regenerative Medicine
AVAN TOKYO Ginza Hair Regenerative Medicine
English / 中文 / Tiếng Việt supported
Inquiries welcomed via DM / LINE / Website / Phone.