

Synovitis as the True Source of Joint Pain: How Stem Cell Conditioned Media Joint Injection May Engage the Inflammatory Cycle2026.07.07
When we see patients complaining of joint pain and swelling, many believe their pain comes purely from worn-down cartilage. However, the true driver of the pain-and-inflammation cycle is often not cartilage itself but an abnormality of the synovial membrane lining the inside of the joint. Synovitis is a hidden inflammatory source behind many joint disorders, including osteoarthritis and rheumatoid arthritis. In this column, Dr. Moriwaki, our supervising physician, outlines how a stem cell conditioned media joint injection may engage this inflammation — its mechanism of action, indications, and limits.
Key Points of This Article
・Synovitis is the true inflammatory source behind pain in many joint disorders of the knee, shoulder, hip, and beyond
・The synovium releases inflammatory cytokines such as IL-1β, TNF-α, and IL-6, which amplify cartilage breakdown and pain signals simultaneously
・Stem cell conditioned media joint injection is being explored along two axes: suppressing inflammation and supporting tissue repair
・It is not a treatment that rebuilds cartilage itself, but a biological approach that acts on the inflammatory environment inside the joint
・Active infection and advanced joint destruction may fall outside indication; understanding limits and individual variation is essential
What Is Synovitis? The Inflammation Happening Inside the Joint
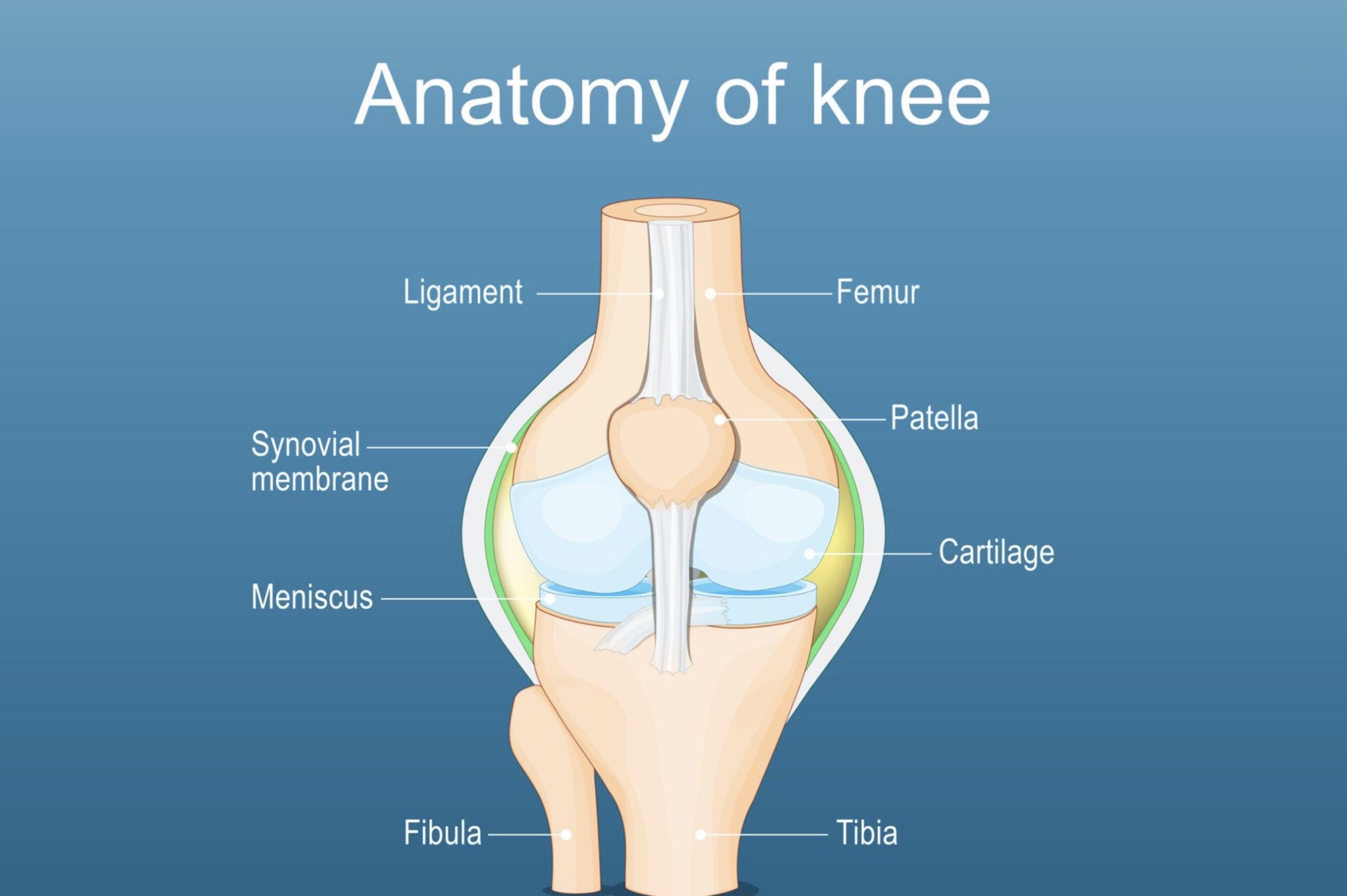
A joint consists of two bones facing each other, enclosed in a sac-like structure called the joint capsule. The inner surface is lined with a thin membrane known as the synovium. The synovium secretes joint fluid (synovial fluid), delivers nutrients to cartilage, and keeps joint motion smooth. When the synovium itself becomes inflamed for any reason, swelling, warmth, pain, and effusion move to the foreground — this state is clinically called synovitis.
Representative Joint Disorders Behind It
The most common background is knee osteoarthritis. Fragments of worn cartilage irritate the synovium, initiating a secondary inflammatory cycle. Other causes include rheumatoid arthritis, gout and pseudogout, septic arthritis, and post-traumatic arthritis. The simplistic idea that “joint pain equals cartilage wear” cannot fully explain what patients experience — inflammation coming from the synovium heavily shapes the intensity of symptoms.
The Joint Inflammatory Cycle and the Pain Mechanism
How synovitis produces pain and functional impairment is not as simple as “it hurts because it is swollen.” Inside the joint, molecules promoting inflammation and molecules promoting repair are constantly competing.
Runaway Inflammatory Cytokines
Inflamed synovial cells release large amounts of inflammatory cytokines such as IL-1β, TNF-α, and IL-6. These induce cartilage-degrading enzymes (MMPs) that drive cartilage breakdown, while simultaneously sensitizing pain neurons and amplifying pain. The synovium behaves as if it is pressing both “the accelerator of cartilage destruction” and “the speaker of pain signals” at the same time.
Increased Joint Fluid and Mechanical Pain
When synovial cells are stimulated, the balance between fluid production and clearance breaks down and fluid accumulates abnormally — the familiar “water in the knee.” Rising intra-articular pressure stretches the joint capsule and mechanically stimulates surrounding nerves. Joint inflammation, therefore, is a source of pain that is both chemical and mechanical.
How Might Stem Cell Conditioned Media Joint Injection Engage Synovitis?
Stem cell conditioned media contains a wide variety of cytokines, growth factors, and exosomes secreted by the cultured stem cells. These are thought to send signals to synovial cells and immune cells in two directions: suppressing inflammation and preparing the tissue repair environment.
Supplying Anti-inflammatory Cytokines from Outside
Basic research reports that conditioned media contains anti-inflammatory molecules such as IL-10 and TGF-β, as well as components that may work to suppress inflammatory signaling. Supplying such anti-inflammatory signals from outside to correct the balance of a runaway cytokine cascade is one conceptual axis of stem cell conditioned media joint injection. However, high-quality comparative trials in humans remain limited, effects vary between individuals, and no definitive efficacy guarantee can be made.
Tissue Repair Signals as the Second Axis
The second axis is the delivery of signals — through growth factors such as TGF-β, IGF-1, and FGF — that may help prepare the repair environment of synovium, cartilage, ligament, and tendon. Joint injection is not a treatment that “rebuilds cartilage itself,” but rather a modality that acts on the cellular environment inside the joint to support the body’s own repair capacity. We should remain cautious about the impression that “a single shot regenerates cartilage.”
Differences from Steroid and Hyaluronic Acid Injections
Steroid injections and hyaluronic acid injections are also options for conservative management of inflammation-related joint pain. Because the mechanisms differ, understanding how stem cell conditioned media joint injection compares helps keep clinical choices grounded. For general information on joint disorders, the Japanese Orthopaedic Association site is a useful reference.
Compared with Steroid Injection
Steroids offer strong anti-inflammatory action that can quickly reduce inflammatory pain and swelling arising from the synovium, but repeated use raises concerns about effects on cartilage and tendons, so frequent injection is not recommended. Conditioned media is expected to work on a different axis — “inflammatory suppression” and “repair-environment support” — so distinguishing purpose and indication is important.
Compared with Hyaluronic Acid Injection
Hyaluronic acid is a physical approach that supplements intra-articular lubrication and viscoelasticity, and has long been used as conservative therapy for knee osteoarthritis. Conditioned media is a biological approach acting on the cellular environment, and the two can be complementary. Considering conditioned media for a knee where hyaluronic acid results have plateaued reflects this difference in mechanism.
Indications and Limits — Who May Benefit and Who Requires Caution
Stem cell conditioned media joint injection is often considered as part of conservative therapy for mild-to-moderate osteoarthritis accompanied by synovitis-related pain and swelling. That said, we cannot expect equivalent results for every kind of joint pain.
Cases Where Benefit Is More Expected
・Osteoarthritis at KL grades I to III with inflammatory pain and swelling as the main symptoms
・A knee that has plateaued on hyaluronic acid but is not yet ready for surgery
・Cases wishing to avoid repeated steroid injections
Cases Requiring Caution or Falling Outside Indication
・KL IV with advanced bony deformity, where total joint replacement is the more reasonable choice
・Active septic arthritis or poorly controlled systemic disease
・Pain that is primarily neural (e.g., sciatica) or from tendon/enthesis outside the joint, not the joint itself
For more on positioning and combination therapy, please see our page on stem cell conditioned media joint injection.
Frequently Asked Questions
Q. Can stem cell conditioned media joint injection completely eliminate the pain of synovitis?
Effects vary between individuals, and complete disappearance of pain cannot be guaranteed. Outcomes depend on the degree of joint degeneration, body weight, activity level, and combination with other treatments. Over several weeks to months, objective evaluation with pain scores and range of motion, together with rehabilitation, orthotics, and lifestyle guidance, is essential.
Q. Does a joint injection cure the joint inflammation itself?
We cannot simply declare that “inflammation completely disappears.” Conditioned media is a treatment that may brake the inflammatory cycle inside the joint and provide signals to prepare the repair environment, but it does not remove the underlying disease such as osteoarthritis or rheumatoid arthritis, so it should be combined with management of the primary disease.
Q. Can it be combined with a steroid injection on the same day?
Because purposes and mechanisms differ, they are usually staggered rather than given at the same moment. Separating the strong anti-inflammatory action of steroids from the inflammation-modulating and repair-supporting role of conditioned media also makes it easier to evaluate results. Discuss timing with your physician.
Q. How many injections are typically needed?
It varies by joint site, disease stage, and goals. Generally, after the first injection, we follow the case for several weeks to months, and decide on additional injections or interval based on changes in pain and range of motion. “More is better” is not the rule; the pros and cons of repeated injections should be discussed with your physician.
Q. Can it be considered for a knee where surgery has been recommended as the only option?
When KL IV bony deformity and joint destruction significantly impair daily life, the benefit obtainable from conditioned media joint injection has clear limits. Total knee replacement may be a more realistic choice, and we will honestly explain the limits of indication.
──────────────
Supervising Physician: Shin Moriwaki, MD
Member, Japan Society of Aesthetic Surgery (JSAS) / Member, American Academy of Aesthetic Medicine
ECFMG Certificate (U.S. Medical License Qualification)
──────────────
📍AVAN TOKYO Ginza Regenerative Medicine
English / 中文 / Tiếng Việt supported
Inquiries welcome via DM / LINE / Website / Phone.