

Subclinical Hypothyroidism and Diffuse Hair Loss in Women — Why Hair Keeps Falling Even When TSH Is Reported “Within Normal Range”2026.07.06
“My thyroid test came back fine, but the hair loss just won’t stop.” — Many women come to the clinic with exactly this concern. Their TSH (thyroid-stimulating hormone) was flagged as “within the reference range” on a routine blood test, so they felt reassured — yet volume slowly declines, and the parting widens over time. Behind this pattern, a subtle hormonal shift called subclinical hypothyroidism is sometimes at work. When free T4 stays within the normal range but TSH sits at the upper end of, or just above, the reference range, this borderline state can quietly underpin diffuse hair loss in women — while being easy to dismiss as “nothing abnormal” if only the number is considered. In this column, we outline how to read these lab values from a supervising physician’s perspective, and where stem cell conditioned media (culture supernatant) fits in as scalp-environment support.
Key Points of This Article
・Subclinical hypothyroidism refers to a borderline thyroid state in which free T4 is normal but TSH is slightly elevated.
・In women with diffuse hair loss, not only overt hypothyroidism but also this borderline abnormality can be a hidden background factor.
・Even when TSH sits inside the reference range, anti-thyroid antibodies, age, and symptoms can change whether observation or treatment is appropriate.
・When subclinical hypothyroidism is suspected, internal medicine evaluation and control should come first — before scalp-side therapy.
・Stem cell conditioned media is not a treatment for the underlying cause; it is best positioned as a complementary approach that supports the scalp environment.
What Is Subclinical Hypothyroidism
A borderline state where “TSH is just a little high”
The thyroid is a small gland at the front of the neck that secretes thyroid hormones (T3, T4) governing whole-body metabolism. Its output is controlled by TSH from the pituitary — when the thyroid slows, TSH rises to push it harder. In overt hypothyroidism, TSH is clearly elevated and free T4 is low. In subclinical hypothyroidism, however, free T4 remains within the normal range while TSH sits slightly high — a borderline band. Because only the numbers are typically checked, this subtle zone is easy to miss.
More common in women, often with chronic thyroiditis behind it
This state is more common in women, especially from middle age onward. In many cases, an autoimmune inflammation such as chronic thyroiditis (Hashimoto’s disease) is quietly affecting the thyroid tissue. When anti-thyroid antibodies (anti-TPO, anti-Tg) are positive, there is a risk of progression to overt hypothyroidism over time. Non-specific symptoms such as fatigue, cold intolerance, constipation, weight gain, and dry skin may accompany hair loss.
Why It Is Linked to Diffuse Hair Loss in Women
Thyroid hormone is a signal that drives the hair cycle
Thyroid hormone is a master regulator of whole-body metabolism, and it also acts on hair follicle cells to drive the hair cycle (anagen → catagen → telogen). When hormone levels fall, hairs that should stay in anagen shift more easily into telogen, producing a diffusely thin, easily-shed pattern typical of diffuse hair loss. Even in subclinical hypothyroidism, long-standing borderline shifts can be associated with a gradual, whole-scalp decline in density.
Overlap with iron deficiency and estrogen fluctuation
In women with diffuse hair loss, the borderline thyroid state is rarely the sole cause. Menstrual iron loss and low ferritin, estrogen fluctuation around menopause, and chronic stress-related telogen effluvium often overlap. A slightly elevated TSH cannot explain everything about the shedding, but ignoring it tends to make other therapies plateau — so it is a factor that deserves attention.
Order of Care and the Role of Stem Cell Conditioned Media
Start with internal medicine evaluation and monitoring
When subclinical hypothyroidism is suspected, the priority is to evaluate anti-thyroid antibodies alongside TSH and free T4, and — considering age and symptoms — decide whether observation or medical treatment is appropriate. How high TSH is, whether antibodies are positive, and whether pregnancy is planned all influence whether close observation is sufficient or a low-dose thyroid hormone replacement should be considered. Once the hormonal baseline is stabilized, the momentum of the hair loss itself often eases. For related reading, see the hair regenerative medicine column archive. General information from a dermatology perspective can also be found at professional societies such as the Japanese Dermatological Association.
A complementary approach to support the scalp environment
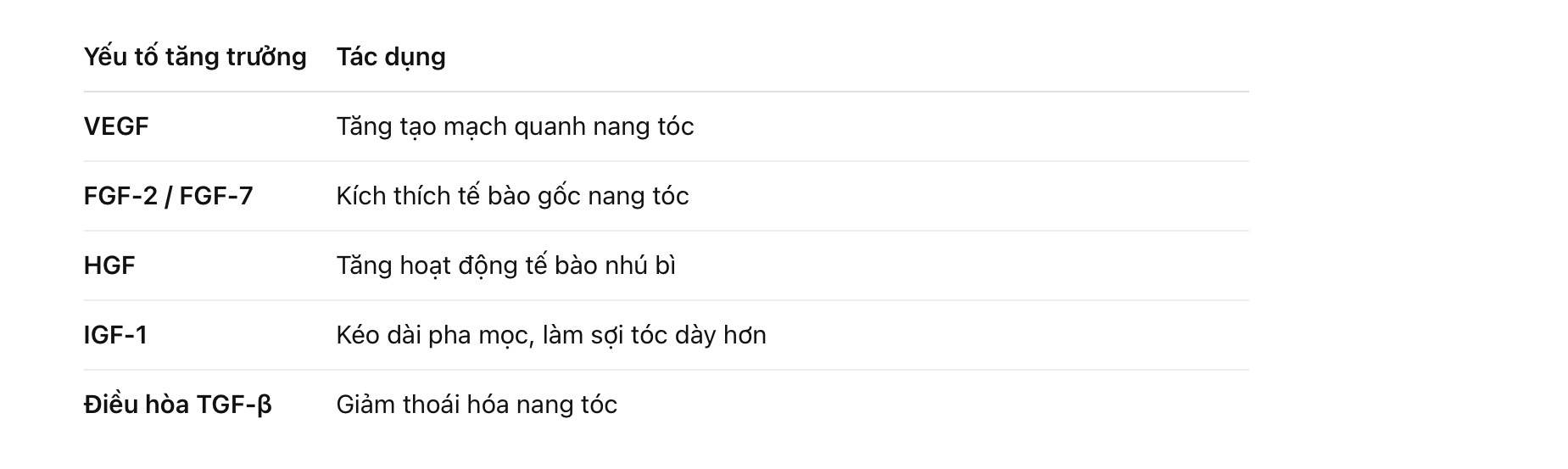
Alongside internal-medicine control, a scalp-side approach can support the follicular environment. Stem cell conditioned media is an umbrella term for the secretions of cultured stem cells — growth factors, cytokines, exosomes, and other bioactive components — delivered by scalp injection or drug-delivery techniques so as to act on the microenvironment surrounding the follicles. It does not treat subclinical hypothyroidism itself, but once medical control has calmed the pace of shedding, it can be designed as a complementary option to support thicker, healthier follicles. Effects vary between individuals, and it must be judged with an honest sense of both indications and limits.
Frequently Asked Questions
Q. My TSH was reported “within the reference range” on my checkup. Should I still consider subclinical hypothyroidism?
If your TSH sat close to the upper limit, or if you have non-hair symptoms such as fatigue or cold intolerance, it is worth re-evaluating together with anti-thyroid antibodies. Judgment is usually made by combining the numbers with symptoms and change over time — not by a single value.
Q. If I get my thyroid under control, will my hair definitely come back?
In overt hypothyroidism, cases of restored density with hormone replacement have been reported. In borderline states or when other factors overlap, however, the degree and timing of improvement vary between individuals. Please understand this is not an area in which a definitive guarantee can be given.
Q. Does stem cell conditioned media treat the thyroid disease itself?
No. Stem cell conditioned media is not a treatment for thyroid disease. It is a complementary option that acts on the scalp environment and the tissue around the follicles — its purpose differs from that of the internal-medicine treatment addressing the underlying cause.
Q. Can I start stem cell conditioned media at the same time as I begin thyroid treatment?
Combination itself is not contraindicated, but layering scalp-side therapy after thyroid control has begun to stabilize typically makes it easier to judge and evaluate the effect of each intervention.
──────────────
Medical supervisor: Shin Moriwaki, MD (supervising physician)
Member, Japan Society of Aesthetic Surgery (JSAS) / Member, American Academy of Aesthetic Medicine
ECFMG certificate holder
──────────────
📍AVAN TOKYO Ginza Hair Regenerative Medicine
AVAN TOKYO Ginza Hair Regenerative Medicine
English / 中文 / Tiếng Việt supported
Inquiries welcome via DM / LINE / Website / Phone.