

Early Signs of AGA Under the Microscope: Reading Hair Diameter Variation and Follicular Unit Density with Stem Cell Conditioned Media2026.07.06
“My hair feels a little thinner lately,” “I notice slightly more hair on the shower drain” — these subtle early signs of hair loss are often hard to judge with a mirror or a photo alone. Androgenetic alopecia (AGA) in particular tends to be noticed only after visible progression, and how early we obtain an objective assessment strongly influences long-term outcomes. At our clinic we perform microscope (trichoscope) evaluation at the very first visit, using “information that the naked eye cannot see” — hair diameter variation, the number of hairs per follicular unit, and peri-follicular inflammation — to judge whether treatment is needed and where stem cell conditioned media fits among the available options.
Key Points of This Article
・Early signs of AGA are hard to catch with the naked eye; microscope-based magnified observation gives an objective measure.
・Hair diameter variation (anisotrichosis) is a hallmark of shortened anagen phase and follicular miniaturization.
・A reduction in the number of hairs per follicular unit suggests entry into telogen and gradual follicular atrophy.
・Stem cell conditioned media is best positioned as a complementary option combined with oral and topical treatments that slow progression.
・Before continuing self-directed scalp care, there is real value in having your scalp “seen under magnification” at a medical facility.
Early Signs of AGA Visible Under the Microscope
Hair Diameter Variation (Anisotrichosis)
On a healthy scalp most hairs are thick anagen hairs of a fairly uniform caliber. Once AGA begins, DHT (dihydrotestosterone) shortens the anagen phase of the hair cycle, and more and more hairs enter telogen before they have had time to fully thicken. Under magnification, extremely fine vellus-like hairs and thick terminal hairs appear together in the same field. This unevenness in thickness is called anisotrichosis, and when more than 20% of hairs show diameter differences, AGA is strongly suspected. The greatest strength of magnified observation is that it can catch this early stage that a mirror simply cannot.
Reduction in Hairs Per Follicular Unit
Hair naturally grows in “follicular units” of two to three hairs sharing one pore. As AGA progresses, these units gradually shift toward single-hair units, so the proportion of pores producing only one hair increases. Counting units on the vertex and comparing them to the occiput under the microscope lets us objectify both the distribution and the stage of AGA. When the occiput is dominated by two- and three-hair units but the vertex is dominated by single-hair units, this is one of the classic patterns of early AGA.
Peri-follicular Inflammation, Sebum and Keratinization
In early AGA, mild peri-follicular findings — erythema and brownish pigmentation around the follicular openings — can also be observed. Excess sebum, abnormal keratinization, dandruff and clogged pores worsen the scalp environment and can blunt the response to the regenerative approaches discussed below, so they should be assessed before layering treatments. Fixing the scalp environment alone will not stop AGA, but stacking treatments without preparing that environment reduces the return on investment.
Where Stem Cell Conditioned Media Fits After the Early Signs Are Caught
First, “Stop the Progression” with Oral and Topical Therapy
Once AGA is confirmed, the first pillar of treatment is progression suppression with 5-alpha reductase inhibitors (finasteride or dutasteride) combined with topical minoxidil for hair growth. This combination is recommended by domestic and international guidelines, and the earlier we start, the more follicles remain and the better the response tends to be. For overall AGA treatment guidance, the guidelines of the Japanese Dermatological Association are one useful reference.
Stem Cell Conditioned Media as a Complementary Option
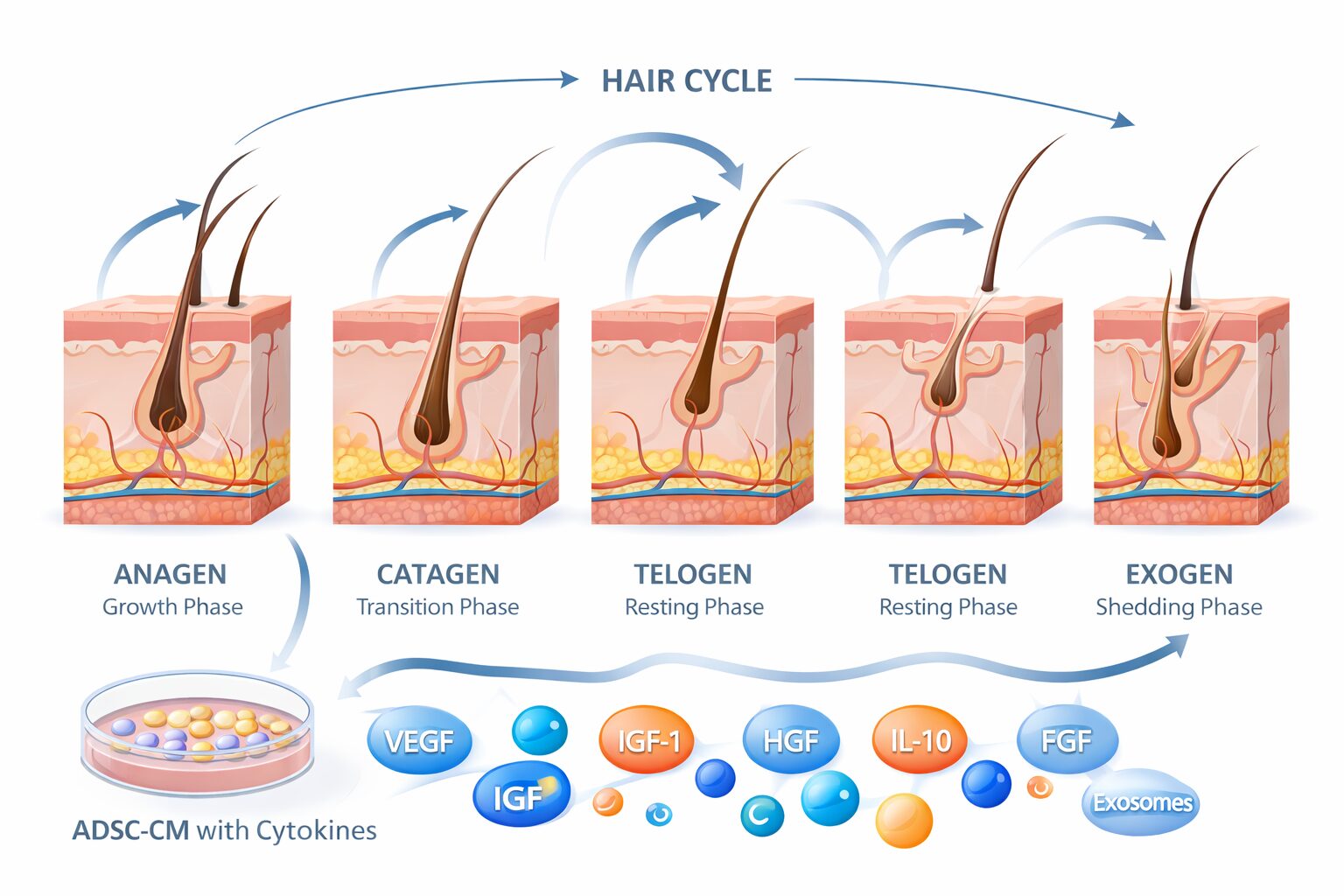
Stem cell conditioned media is a regenerative therapy in which the complex of growth factors, cytokines and exosomes secreted by mesenchymal stem cells is delivered to the scalp to act on the peri-follicular microenvironment. It is not, on its own, a drug that “cures AGA at its root,” but combined with oral and topical treatments it is expected to complement follicular angiogenesis, anti-inflammatory action, and signals that extend the anagen phase. Especially at the stage where the microscope shows “diameter variation is starting to stand out but follicular units are still preserved,” a protocol combining oral progression suppression with local complementation is a reasonable option. That said, in end-stage cases where follicles have already fully atrophied the response is limited, and we make sure to share honestly that individual differences and clear limits exist.
Objectify Response with “Magnified Photographs”
After starting treatment, we photograph the same sites under the microscope every three to six months and objectively track diameter variation, hairs per follicular unit, and the thickening of vellus hairs. Relying on “I feel like it increased / I feel like nothing changed” makes it too easy to waver on continue-or-stop decisions. We use the same yardstick when this treatment has been introduced, and when the response is limited we review injection intervals, injection depth and concomitant medication. For related topics on scalp environment and regenerative medicine, please see the list of related articles on hair regenerative medicine.
Frequently Asked Questions
Q. Can a microscope exam alone confirm whether I have AGA?
Diameter variation and reduced follicular units strongly suggest AGA, but confirming the diagnosis requires combining these findings with history, family history, progression speed and blood work (thyroid, ferritin, and prolactin in women, etc.). It is essential to rule out telogen effluvium, autoimmune alopecia, nutritional alopecia and other non-AGA causes.
Q. Is a microscope exam worthwhile even when hair loss is still mild?
The “still-not-worried” stage is precisely when microscope evaluation is most valuable. If diameter variation is just beginning, there is a good chance of halting progression with oral and topical therapy, and complementary options such as conditioned media treatment come into play. The earlier we look, the more follicles remain and the wider the treatment menu that can be offered.
Q. Can hair grow with stem cell conditioned media alone?
Stem cell conditioned media works by improving the peri-follicular environment and supplementing growth factor signals. It is best understood as a complementary treatment that shows its strength combined with oral and topical therapy, rather than as a monotherapy. Response and indications vary between individuals, and in rapidly progressing AGA or cases with few remaining follicles the effect is limited.
Q. How long before we assess whether it is working?
Because the hair cycle runs on a scale of months, we typically re-evaluate at three, six and twelve months after starting, using magnified microscope images to trace the course. Taking a longer, hair-cycle-aware interval also helps avoid misjudging early shedding right after starting as “not working.”
Q. I have already been told at another clinic that I have AGA. Is there any point being examined again?
Yes. Magnified observation makes changes in diameter variation and follicular units visible, so you can objectively check whether the current treatment is working. If the response is limited, it becomes useful material for reviewing the oral regimen, adding conditioned media treatment, or re-evaluating lifestyle factors.
──────────────
Medical Supervisor: Shin Moriwaki, MD
Member, Japanese Society of Aesthetic Surgery (JSAS) / Member, American Academy of Aesthetic Medicine
ECFMG Certificate (US medical qualification)
──────────────
📍AVAN TOKYO 銀座 毛髪再生医療
AVAN TOKYO Ginza Hair Regenerative Medicine
English / 中文 / Tiếng Việt supported
Inquiries welcome via DM / LINE / Website / Phone.