
Are Gray Hair and Thinning the Same Problem? — Aging of Hair Follicle and Melanocyte Stem Cells, and Stem Cell Conditioned Media2026.05.31
“My gray hairs keep increasing,” “I feel my hair volume has dropped too” — these are concerns frequently raised together by patients in their 40s and beyond. Most people view gray hair and thinning as entirely separate issues, yet inside the hair follicle the very same process — aging — is unfolding. Stem cell conditioned media, an option that has drawn increasing attention in regenerative medicine, is being studied as a new way to act on this shared foundation.
This column organizes the underlying mechanisms of gray hair and thinning from the perspective of the “aging of two stem cell populations,” and explains how stem cell conditioned media may intervene, drawing on AVAN TOKYO’s clinical viewpoint.
Are gray hair and thinning really “separate problems”?
Gray hair is a color issue; thinning is a matter of density or shaft thickness — viewing them this way is entirely natural. But when we look at the histological structure of the hair follicle, both are supported, within the same follicular unit, by two distinct stem cell populations.
Two stem cells coexisting in one follicle
In the region called the “bulge” of the follicle, hair follicle stem cells — responsible for hair growth — and melanocyte stem cells — the source of the pigment-producing melanocytes — live side by side.
Hair growth begins when hair follicle stem cells become active and differentiate into matrix cells.
Meanwhile, the color of the hair shaft is supplied by melanocytes that originate from melanocyte stem cells.
In short, two lineages — “stem cells that build the hair” and “stem cells that color the hair” — sit together in a single follicle.
“Aging” as the shared trigger
What happens with age is a decline in the function of these stem cells.
Their numbers do not suddenly drop to zero; rather, they enter dormancy or lose self-renewal capacity, so the follicle’s output gradually diminishes.
When this change predominates in hair follicle stem cells it manifests as thinning, and when it predominates in melanocyte stem cells it manifests as gray hair — but the underlying structure of “stem cell exhaustion” is essentially the same.
Depletion of hair follicle stem cells drives thinning
Viewing what happens in AGA or diffuse hair loss at the level of hair follicle stem cells changes the picture significantly.
Stem cells do not “disappear” but “stop working”
For a long time, thinning was explained as “a disease in which the follicle itself disappears,” but recent research reports that the bulge-area hair follicle stem cells are relatively preserved even in AGA-affected scalp.
The problem is that these stem cells become poorly mobilized toward their differentiation target — the matrix lineage.
One leading interpretation today is that the “exit” has narrowed, while the stem cells themselves remain in place.
This is precisely why the realistic goal of thinning treatment is shifting from “rebuilding lost follicles” to “restarting stem cells that have stopped moving.”
Chronic microinflammation and cellular senescence
The biggest culprit halting stem cell function is long-running microinflammation in the scalp.
Inflammatory cytokines generated by sebum oxidation, UV exposure, and lifestyle stress damage the stem cell niche (the microenvironment where stem cells live) and accelerate cellular senescence.
This is consistent with the broader trend of managing the entire scalp — including its inflammatory and metabolic environment — reflected in the AGA treatment guidance of the Japanese Dermatological Association.
It is not only about suppressing hormone pathways with oral drugs; improving the inflammatory environment of the scalp itself has become an increasingly important perspective.
Depletion of melanocyte stem cells drives gray hair
Gray hair is not simply “visible aging”; histologically it can be described as a quite distinct cellular event.
Early loss of melanocyte stem cells
It is known that melanocyte stem cells have a shorter lifespan than hair follicle stem cells.
Normally, with each follicular cycle, melanocyte stem cells self-renew while a portion differentiates into melanocytes that deposit pigment into the hair.
However, with aging and accumulated oxidative stress, the balance between self-renewal and differentiation breaks down, biased toward differentiation, so the stem cell pool itself can be exhausted earlier.
This is one reason why, for some people, gray hair becomes prominent before thinning does.
Accumulated oxidative stress and DNA damage
UV light, smoking, psychological stress, chronic lack of sleep.
What these have in common is that they all increase reactive oxygen species inside the follicle.
Reactive oxygen species damage DNA, and when repair cannot keep up, melanocyte stem cells are pushed toward apoptosis or forced differentiation.
Behind complaints of “a sudden surge in gray hair,” such concentrated oxidative stress is often hidden.
How does stem cell conditioned media intervene?
Given the aging of hair follicle and melanocyte stem cells described above, what can stem cell conditioned media be expected to do?
An “alarm clock” for dormant stem cells
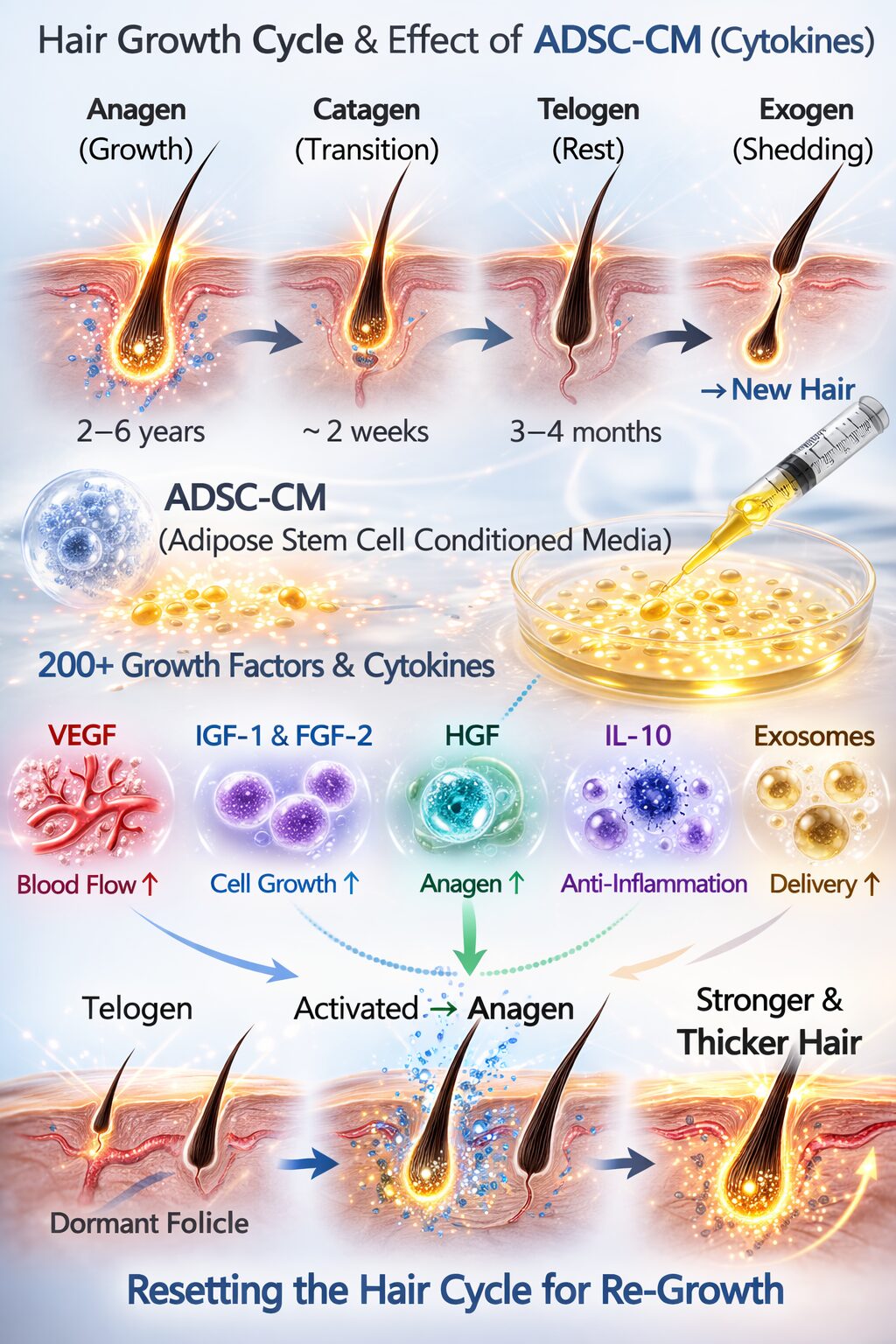
Stem cell conditioned media contains many types of growth factors — including FGF, VEGF, and IGF — along with exosomes, the representative carriers of intercellular signaling.
These are thought to deliver signals to the niche of dormant stem cells and act as an “alarm clock” that returns them to the differentiation cycle.
In particular, the mobilization of bulge-area hair follicle stem cells toward differentiation is expected, and we are seeing more cases in borderline patients — AGA, diffuse thinning, postpartum hair loss — where clinical change becomes noticeable.
Anti-inflammation and angiogenesis — “rebuilding the environment”
Another strength of stem cell conditioned media is its anti-inflammatory and angiogenic action.
As scalp microcirculation improves and chronic hypoxia and undernutrition are relieved, both hair follicle stem cells and melanocyte stem cells gain an environment that is easier to live in.
For patients struggling with thinning and gray hair simultaneously, this is a highly rational approach because it acts on the shared foundation of both.
What we have seen in AVAN TOKYO’s clinical practice
In actual clinical practice, combining with Morpheus8 drug delivery makes it possible to deliver stem cell conditioned media uniformly to deeper layers.
Patients with “only thinning” or “only gray hair” are actually a minority; most carry both concerns at the same time.
Once we understand that both share the same root — “stem cell aging” — treatment design naturally shifts from “hitting each symptom” to “rebuilding the foundation.”
For more treatment cases and related topics, please also see our collection of related columns on hair regenerative medicine.
──────────────
【監修】森脇 進 / Shin Moriwaki(監修医師)
日本美容外科学会(JSAS)会員 / American Academy of Aesthetic Medicine 会員
米国医師免許資格(ECFMG certificate)
──────────────
📍AVAN TOKYO 銀座 毛髪再生医療
AVAN TOKYO Ginza Hair Regenerative Medicine
English / 中文 / Tiếng Việt 対応可能
ご相談は DM / LINE / Website / Phone より承っております。