

When Imaging Shows No Abnormality Yet Your Back Still Hurts — How Dr. Moriwaki Diagnoses Lumbar Facet Joint Syndrome and Positions Stem Cell Conditioned Media Joint Injection2026.07.12
“My back hurts, but the orthopedic X-ray showed no abnormality.” Many patients share this experience. One of the most easily overlooked causes is lumbar facet joint syndrome. When inflammation or degeneration of the small joints behind the lumbar spine underlies chronic low back pain, standard X-rays and early MRI may not capture a clear finding. From the perspective of Dr. Moriwaki at AVAN TOKYO Ginza Regenerative Medicine, this article organizes how lumbar facet joint syndrome is assessed and how stem cell conditioned media joint injection is positioned as one option.
Key Points of This Article
・Lumbar facet joint syndrome involves inflammation or degeneration of the small posterior joints of the lumbar spine and may not appear on imaging, making it easy to overlook
・The pattern is pain worsening on backward extension or same-side lateral bending, along with localized tenderness over the facet joint level of the paraspinal region
・Diagnosis centers on history and physical examination, with a selective facet joint block used when needed to confirm the pain source
・Stem cell conditioned media joint injection is one conservative option targeting the inflammatory environment, but its effect cannot be guaranteed
・Progressive leg numbness, urinary disturbance, or advancing muscle weakness call for immediate orthopedic reassessment as the top priority
Lumbar Facet Joint Syndrome Behind the “No Abnormality on Imaging” Back Pain
The lumbar spine is supported in a three-point structure formed by the vertebral body, intervertebral disc, and the posterior facet joints. The facet joints are paired synovial joints that carry both mobility and stability of the lumbar spine. Like any synovial joint, they possess cartilage, a joint capsule, and synovium. In other words, they are “joints” like the knee or shoulder and can undergo degeneration and inflammation.
Why It Is Hard to See on Imaging
In early stages, bone spurs and narrowing of the joint space on plain X-ray may not yet be clear. Depending on MRI protocols and reading perspective, inflammation of the joint capsule or subtle cartilage change may not be reported as “abnormal.” When no large structural lesion such as a disc herniation or spinal canal stenosis coexists, the images are often described as “age-appropriate,” leaving patients caught in the dilemma of “pain with no abnormality.”
Typical Pain Presentation
A key clue to lumbar facet joint syndrome is strong movement-dependence of the pain. Pain provoked or intensified by backward extension or same-side lateral bending, marked morning stiffness that eases somewhat with movement, and worsening with prolonged standing or walking — these features suggest joint-origin pain. Focal tenderness may also be reproduced by pressing over the facet joint level of the paraspinal muscles.
How to Identify Joint-Origin Pain When Imaging Is “Normal”
Rather than depending on imaging, the essential attitude is to build a picture of the pain source from history and examination.
Distinguishing from Neurogenic Pain
When radiating numbness or electric shock-like pain in the leg is strong, disc herniation and spinal canal stenosis — neural-origin conditions — are considered first. Sciatica-like pain spreading from the buttock down the leg often reflects nerve root or cauda equina compression rather than the joint itself, and must be separated from what a joint injection can target.
Diagnostic Blocks as a Confirmatory Tool
When facet joint origin is clinically suspected, a selective block delivering a small volume of local anesthetic into the facet joint or medial branch nerve can confirm the pain response. If pain eases immediately after injection, that joint is more likely to be the primary source. For information on joint disorders, referring to the guidance of the Japanese Orthopaedic Association is also useful. Confirming “whether the pain is joint-origin” is the starting point for designing treatment.
Stem Cell Conditioned Media Joint Injection as an Option for Lumbar Facet Joint Syndrome
Once the assessment points to facet joint origin, stem cell conditioned media joint injection becomes a candidate among conservative options.
Targeting the “Inflammatory Environment”
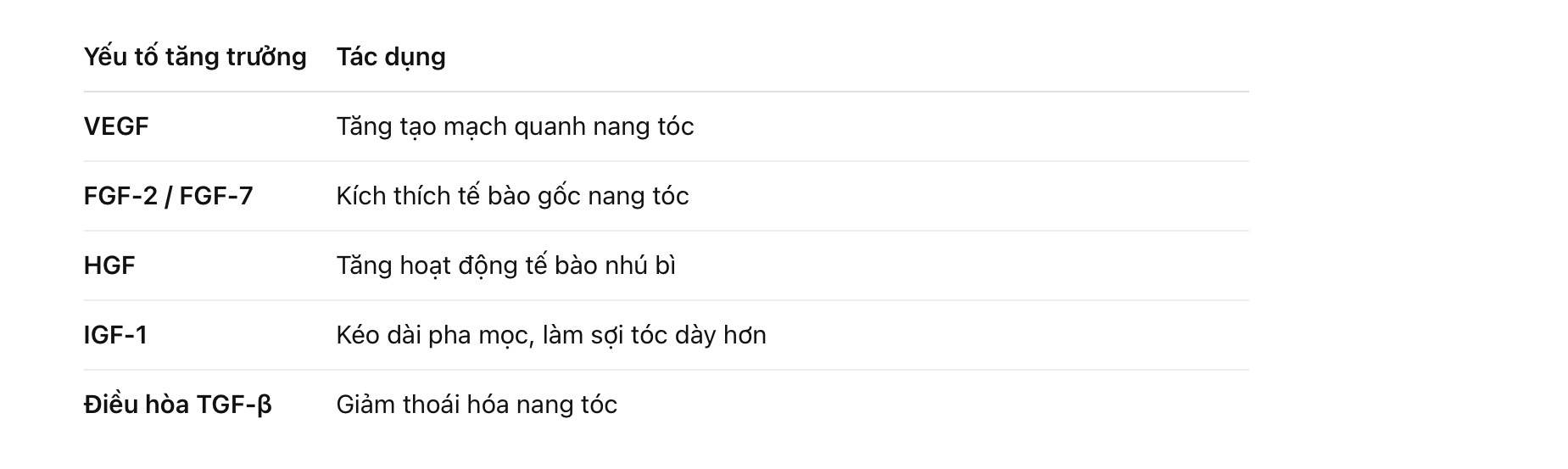
Stem cell conditioned media is reported to contain multiple growth factors and anti-inflammatory cytokines such as TGF-β, IGF-1, and FGF. Because chronic joint pain involves synovitis and capsular inflammation, this protein mix is expected to act on the inflammatory cycle and moderate the local environment. It is, however, not a treatment that “fully regenerates the cartilage itself.” Its position is that of a conservative therapy aimed at the inflammatory environment underlying the pain.
Honest About Both Effect and Limits
Individual response varies, and pain change must be tracked over weeks to months. Effect is judged objectively by pain score, range of motion, and daily activity. When response is poor, we shift to continuing, modifying, or returning to orthopedic reassessment. This is not a treatment that stands alone without a foundation of exercise therapy, core stabilization, and review of posture and daily movement. Details of the treatment framework are available at our page on stem cell conditioned media joint injection.
There Are People For Whom It Is Not Suitable
Progressive leg numbness or weakness and bladder/bowel disturbance suggest emergency conditions such as cauda equina syndrome, and orthopedic imaging reassessment and specialized intervention take priority. Active infection, poorly controlled systemic disease, and use of anticoagulants also require careful judgment. We explain from the first visit that this is not a first-line treatment for everyone.
Frequently Asked Questions
Q. I was told imaging showed no abnormality — is it really lumbar facet joint syndrome?
Imaging findings and pain sources do not always align. Early changes of this condition are hard to capture on imaging, so we judge from history, examination, and response to diagnostic block. Carefully confirming how your pain reproduces with movement matters.
Q. Does stem cell conditioned media joint injection cure lumbar facet joint syndrome?
It is not a treatment that guarantees cure. It is one conservative option aiming to act on the periarticular inflammatory environment. Response varies among individuals, and realistic management combines it with exercise therapy and lifestyle review.
Q. How long is needed to judge effect?
We track changes in pain, range of motion, and daily activity over weeks to months. If response is poor, we shift to continuation, change, or orthopedic reassessment.
Q. How is it used alongside other treatments?
Existing conservative therapies such as exercise therapy, medication, and nerve block form the foundation. Because steroid local injection and hyaluronic acid have different aims and mechanisms of action, combinations and sequencing are considered based on condition.
Q. Are there conditions in which injection should be avoided?
If leg numbness or weakness is progressing, if there is bladder/bowel disturbance, or if fever or signs of infection are present, injection is postponed and orthopedic reassessment takes priority.
──────────────
Supervising physician: Shin Moriwaki, MD
Member, Japan Society of Aesthetic Surgery (JSAS) / Member, American Academy of Aesthetic Medicine
ECFMG certificate (US medical qualification)
──────────────
📍AVAN TOKYO 銀座 再生医療
AVAN TOKYO Ginza Regenerative Medicine
English / 中文 / Tiếng Việt supported
Inquiries welcome via DM / LINE / Website / Phone.